Clenbuterol (Clenbuterol, “maple”) is a drug used medically to treat bronchial asthma. In recent years, clenbuterol has found widespread use in bodybuilding and fitness due to its ability to burn fat, so it is often used by athletes for weight loss and leaning. Courses of clenbuterol often include thyroxine and ketotifen to speed up the weight loss process. Clenbuterol is not related to anabolic steroids and belongs to the group of adrenomimetics, which have their physiological effect by stimulating the beta-2-adrenoceptors, which activates the sympathetic nervous system and triggers lipolysis. A prescription is required to purchase the drug.
It can be prescribed for girls without the risk of androgenic side effects common to anabolic steroids.
Half-life: 36 hours

Doping Status
Clenbuterol has been banned by WADA for use in sports since 1992. Standard anti-doping tests usually respond to a concentration of 5-10 ng/L in the urine, which is seen 4-5 days after the last dose. More sensitive tests extend the detection time of clenbuterol to 2-3 weeks or longer (1-2 ng/L). The drug accumulates in adipose tissue and may be more actively released during exercise or competition.
One possible route for clenbuterol to enter the athlete’s body could be through meat, as in some countries (China, Mexico) it is used to increase the weight of fattened animals.
Several scientific articles have reported the frequent inappropriate inclusion of clenbuterol in fat burning sports supplements.
Mechanism of Action
As a beta-2 agonist, clenbuterol acts as a fat burner by binding to the type 2 beta receptors in human fat and muscle tissue. After clenbuterol binds to the receptor, it triggers a cascade of biochemical reactions leading to increased synthesis of cAMP (cyclic adenosine monophosphate). cAMP in turn activates enzymes that mobilize fatty acids from adipocytes (fatty tissue cells).
The action of clenbuterol on the beta-2-adrenoceptors of presynaptic membrane increases the release of noradrenaline and adrenaline, which have a powerful fat-burning effect. Clenbuterol increases basal metabolic rate by 20-30% from baseline.
Clenbuterol inhibits lipoprotein lipase activity, as a result fat deposition in adipose tissue becomes impossible. By acting on beta-2-adrenoceptors in the central nervous system, this drug increases the secretion of thyroid hormones – the body’s natural fat burners.
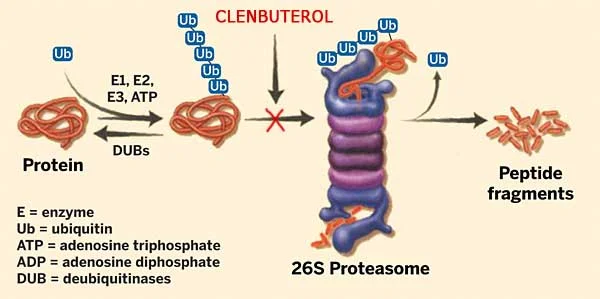
The unique feature of clenbuterol is that it is not only a powerful fat burner, but also has a strong anti-catabolic effect, protecting muscles from degradation, which is very important during weight loss and lean bodybuilding. Studies have found that the anti-catabolic action of the drug is due to the blocking of Ca2+ dependent and ubiquitin-proteasome proteolysis.
A 2012 study (Francesca Wannenes, Loretta Magni) confirms the ability of clenbuterol to block muscle atrophy mechanisms. A new 2014 study showed that β-agonists (catecholamines) released during intense exercise induce CREB-mediated transcription through activation of its obligate coactivators CRTC2 and Crtc3.
In contrast to the catabolic activity normally associated with sympathetic nervous system function, activation of Crtc/Creb proteins in the skeletal muscles of transgenic mice results in enhanced anabolic processes and increased protein synthesis. Thus, in animals with CRTC2 overexpression, the cross-sectional area of myofibrils increases, intramuscular triglycerides and glycogen content increase. In addition, there is a significant increase in the strength indices.
Due to the above mentioned mechanisms, the compound has a moderate anabolic effect, which has been proven in human trials and practical application in bodybuilding.
Given that the drug has almost no interaction with beta-1-adrenoceptors, there is bronchial dilation and respiratory relief and a much lower incidence of side effects on the cardiovascular system compared to non-selective agonists such as ephedrine.
Human Studies
A 2015 study by Lee P. 2015 was the first reliable proof of the efficacy of beta-agonists in humans. Formoterol (β2 selective agonist), an analogue by mechanism of action, at a dose of 160 mcg/day, stimulated anabolism and increased protein synthesis without causing cardiovascular side effects, while these effects were more pronounced in girls.
In addition, Morten Hostrup (2015) found that the beta-2-adrenomimetic terbutaline (10-15 mg/day) caused a statistically significant increase in lean muscle mass, increased strength and endurance during maximum exercise on the exercise bike.
Effects of clenbuterol
- Fat burning and muscle drying
- Increased strength and endurance
- Increase in temperature
- Appetite reduction
- Mental activation
- Anti-catabolic effect
- Anabolic action
The low frequency of side effects (practice shows that irreversible side effects are almost completely absent) and a wide range of positive effects make clenbuterol one of the best fat burners in bodybuilding.
Some authors (Yuri Bombela) claim that in high doses clenbuterol may have catabolic effects, but this is not true in the absence of any physiological or empirical substantiation.
A course of clenbuterol: weight loss
In men, the recommended dose of clenbuterol for drying and weight loss is 120-140 mcg per day. For women, the average dose of clenbuterol for drying and weight loss is 80-100 mcg per day. The course of clenbuterol has its own subtle features, which must be strictly followed to avoid side effects.
The duration of a course of clenbuterol is usually 2 weeks, then habituation (receptor tolerance) develops and effectiveness decreases. After that it is necessary to take a 2 week break with ketotifen, without it the break is useless, and then repeat the course; without ketotifen the break should be much longer. The need for a break was scientifically substantiated back in 1990: Desensitization of beta-adrenoreceptors develops through receptor phosphorylation and through other biochemical modifications at the level of secondary messengers (kinases, G-proteins, etc.). It takes several days to update these structures.
The duration and effectiveness of a course of clenbuterol, as mentioned, can be increased by including ketotifen. Sometimes a pulse course is recommended to prevent receptor adaptation – 2 days on, 2 days off, but this regimen is less effective.
Don’t forget to take enough protein, BCAA’s and other cortisol blockers during the cycle, this will greatly improve the results. Follow an appropriate diet for weight loss or drying off.
A 2010 study found a synergistic effect when combined with anabolic steroids, which confirms the advisability of including the drug at the end of the AC course. Many experts do not recommend combining the drug with anabolic steroids, because the risk of cardiac hypertrophy increases.
Course of clenbuterol without ketotifen
- day 1: 20 micrograms (0.02 mg)
- day 2: 40 micrograms (0.04 mg)
- day 3: 60 micrograms (0.06 mg)
- day 4: 80 micrograms (0.08 mg)
- day 5: 100 micrograms (0.10 mg)
- day 6-12: 120 mcg (0.12 mg)
- day 13: 80 micrograms (0.08 mg)
- day 14: 40 microgram (0.04 mg)
- break
The dose of clenbuterol should increase progressively during the first week. The optimal time to take clenbuterol is in the morning, so as not to cause insomnia, and the effectiveness of the drug is higher in the morning hours. If you increase the dosage, start taking it in 2 doses: in the morning and in the afternoon.
A course of clenbuterol + ketotifen
Ketotifen is an anti-allergic agent with the unique ability to restore the sensitivity of beta-2-adrenoreceptors to clenbuterol. This property has been repeatedly proven in studies involving not only asthma patients but also isolated lymphocytes. The mechanism of this effect is obviously not related to histamine receptors but to inhibition of phosphodiesterase,[16] which regulates the cAMP-dependent metabolism of all cells, allowing the results obtained in work with lymphocytes to be extrapolated to adipose tissue.
Similar receptor resensitization effects have been observed with ketotifen for other beta-agonists, as confirmed by a large number of studies.
Ketotifen can be used to speed up the weight loss or weight loss process by 10 to 20 percent and extend the course by up to 8 weeks. On top of that, ketotifen can help eliminate mental agitation, limb tremors, insomnia and heart palpitations.
- day 1: 20 mcg clenbuterol
- day 2: 40 mcg clenbuterol
- day 3: 60 mcg clenbuterol
- day 4: 80 micrograms clenbuterol
- day 5: 100 mcg clenbuterol + 1 mg ketotifen
- day 6-27: 120 mcg clenbuterol + 2 mg ketotifen
- day 28: 80 mcg clenbuterol + 2 mg ketotifen
- day 29: 50 mcg clenbuterol + 1-2 mg ketotifen
- day 30: 33-35 mcg clenbuterol + 1 mg ketotifen
- at least two weeks break
Ketotifen is taken at night, clenbuterol in the morning. The dosage distribution is the same as in the previous example.
Combination: To maximize the effectiveness of the course, clenbuterol is combined with thyroxine. However, in this case there is an increased risk of side effects.
Side effects of clenbuterol
The side effects of clenbuterol are listed by frequency of occurrence:
- Heart palpitations (60%) – resolved by beta-1-adrenoblockers. Take 5 mg of Bisoprolol or 50 mg of Metoprolol in the morning.
- Shivering (20%) – especially pronounced on the first day of administration, then gradually subsides. It is relieved by ketotifen.
- Sweating (10%)
- Insomnia (7%) – relieved by ketotifen
- Restlessness (6%) – relieved by ketotifen
- Increased blood pressure (6%) – resolved by beta-1-adrenoblockers. Take 5 mg of Bisoprolol or 50 mg of Metoprolol in the morning.
- Stool disturbance – diarrhea (5%) – usually seen only in the first few days of taking the drug
Nausea (3%) - Seizures (in case of an overdose or during the initial stages of taking the drug)
- In individual cases, headache may occur, most likely related to an increase in blood pressure.
As you can see, many of the side effects of clenbuterol can be prevented with ketotifen and bisoprolol (metoprolol). Also, it should be noted that most side effects are particularly pronounced only in the initial stages of the course, and after a few days they subside or disappear completely.
It has been shown in animal experiments that large doses of clenbuterol can be toxic to the myocardium, and testicular tissue.
In Ostapenko’s book Anabolic Drugs, there is information that due to the accumulation of polyamines in cells, clenbuterol can cause malignancy and lead to enlargement of internal organs (particularly myocardial hypertrophy), which can explain the pronounced bulging of the anterior abdominal wall in many modern athletes. However, there is no scientific and practical confirmation of these statements, so they can be regarded only as the author’s conjectures. In addition, it has been determined that the abdominal enlargement in professional athletes is primarily related to the use of high doses of growth hormone.
Beta 2 receptors are also found in the kidneys which results in increased renin secretion, which then leads to potassium excretion from the body, therefore additional asparkam administration is considered advisable.
Clenbuterol slightly increases insulin secretion. Acting on the intestinal receptors, it causes its relaxation, which may affect its function: incomplete digestion of food, diarrhea, flatulence, dysbacteriosis.
The information in some instructions about bronchospasm after withdrawal is only relevant for people with asthma who have an increased bronchial response.
Caffeine, yohimbine, thyroxine, and other stimulants significantly increase the frequency of side effects.
Clenbuterol and alcohol
It is not recommended to combine clenbuterol and alcohol, as it may increase nausea and heart palpitations. Clenbuterol and alcohol increase the strain on the cardiovascular system. In addition, alcohol interferes with weight loss and leaning. Alcohol destroys muscle. Read the main article: alcohol and muscle.